

Technology has been a boon to healthcare. Minimally-invasive procedures have significantly increased safety and recovery time of surgeries. Global collaboration between doctors has improved diagnosis and treatment. Rise in awareness of patients has increased the demand for good quality healthcare services. These improvements, coupled with the growing penetration of IT infrastructure, are generating huge volumes of digital health data in the country.
However, healthcare in India is diverse and fragmented. During an entire life cycle, an individual is served by numerous healthcare providers, of different sizes, geographies, and constitutions. The IT systems of different providers are often developed independently of each other, without adherence to common standards. This fragmentation has the undesirable consequence of the systems communicating poorly, fostering redundant data collection across systems, inadequate patient identification, and, in many cases, privacy violations.
We believe that this can be addressed through two major steps. Firstly, open standards have to be established for health data collection, storage, sharing and aggregation in a safe and standardised manner to keep the privacy of patients intact. Secondly, patients should be given complete control over their data. This places them at the centre of their healthcare and empowers them to use their data for value-based services of their choice. As the next wave of services is built atop digital health data, data protection and empowerment will be key to transforming healthcare.
Numerous primary health care services are already shifting to smartphones and other electronic devices. There are apps and websites for diagnosing various common illnesses. This not only increases coverage but also takes the burden away from existing infrastructures which can then cater to secondary and tertiary services. Data shared from devices that track steps, measure heartbeats, count calories or analyse sleeping patterns can be used to monitor behavioural and lifestyle changes – a key enabler for digital therapeutic services. Moreover, this data can not only be used for monitoring but also for predicting the onset of diseases! For example, an irregular heartbeat pattern can be flagged by such a device, prompting immediate corrective measures. Thus, we see that as more and more people generate digital health data, control it and utilise it for their own care, we will gradually transition to a better, broader and preventive healthcare delivery system.
In this context, we welcome the proposed DISHA Act that seeks to Protect and Empower individuals in regards to their electronic health data. We have provided our feedback on the DISHA Act and have also proposed technological approaches in our response. This blog post lays out a broad overview of our response.
As our previous blog post articulates the principles underlying our Data Empowerment and Protection Architecture, we have framed our response keeping these core principles in mind. We believe that individuals should have complete control of their data and should be able to use it for their empowerment. This requires laying out clear definitions for use of data, strict laws to ensure accountability and agile regulators; thus, enabling a framework that addresses privacy, security and confidentiality while simultaneously improving transparency and interoperability.
While the proposed DISHA Act aligns broadly with our core principles, we have offered recommendations to expand certain aspects of the proposal. These include a comprehensive definition of consent (open standards, revocable, granular, auditable, notifiable, secure), distinction between different forms of health data (anonymization, deidentification, pseudonymous), commercial use of data (allowed for benefit but restricted for harm) and types and penalties in cases of breach (evaluation based on extent of compliance).
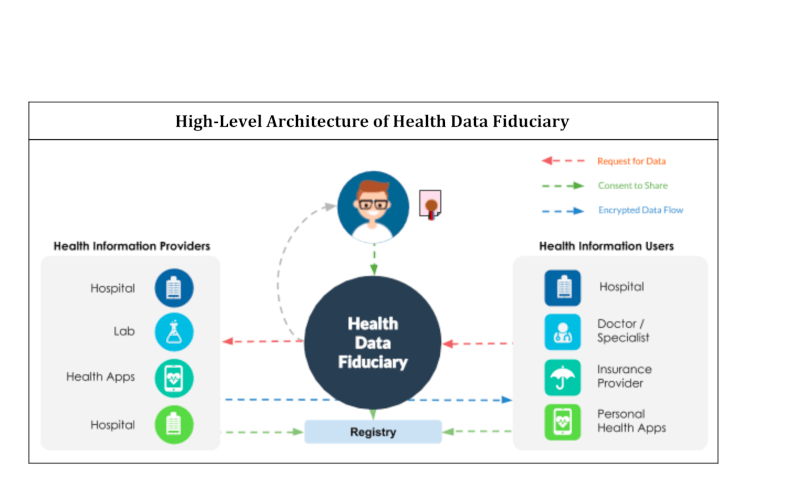
Additionally, we have outlined the technological aspects for implementation of the Act. We have used learnings from the Digital Locker Framework and Electronic Consent Framework (adopted by RBI’s Account Aggregator), previously published by MeitY. This involves the role of Data Fiduciaries – entities that not only manage consent but also ensure that it aligns with the interests of the user (and not with those of the data consumer or data provider). Data Fiduciaries only act as messengers of encrypted data without having access to the data – thus their prime task remains managing the Electronic Data Consent. Furthermore, we have highlighted the need to use open and set standards for accessing and maintaining health records (open APIs), consented sharing (consent framework) and maintaining accountability and traceability through digitally verified documents. We have also underscored the need for standardisation of data through health data dictionaries, which will open up the data for further use cases. Lastly, we have alluded to the need to create aggregated anonymised datasets to enable advanced analytics which would drive data-driven policy making.
We look forward to the announcement and implementation of the DISHA Act. As we move towards a future with an exponential rise in digital health data, it is critical that we build the right set of protections and empowerments for users, thus enabling them to become engaged participants and better managers of their health care.
We have submitted our response. You can find the detailed document of our response to DISHA Act below